The Science of Testosterone Replacement Therapy (TRT): Clinical Benefits, Protocols, and Performance Optimization
By Genivra Labs Research Team
Testosterone Replacement Therapy (TRT) has evolved from a niche medical treatment for severe hypogonadism into a cornerstone of modern longevity, men’s health, and performance optimization. As our understanding of endocrinology deepens, the clinical data overwhelmingly supports the profound impact that optimized testosterone levels have on nearly every physiological system in the male body.
At Genivra Labs, we approach hormone optimization through the lens of rigorous science. This comprehensive guide explores the evidence-based benefits of TRT, the mechanisms of the Hypothalamic-Pituitary-Testicular Axis (HPTA), modern dosing protocols, and how strategic peptide stacking can amplify therapeutic outcomes.

Understanding the HPTA Axis and Testosterone Decline
Testosterone is the primary male sex hormone, responsible for maintaining bone density, fat distribution, muscle strength, red blood cell production, and sexual function . It is produced primarily in the testes, regulated by a complex feedback loop known as the Hypothalamic-Pituitary-Testicular Axis (HPTA).
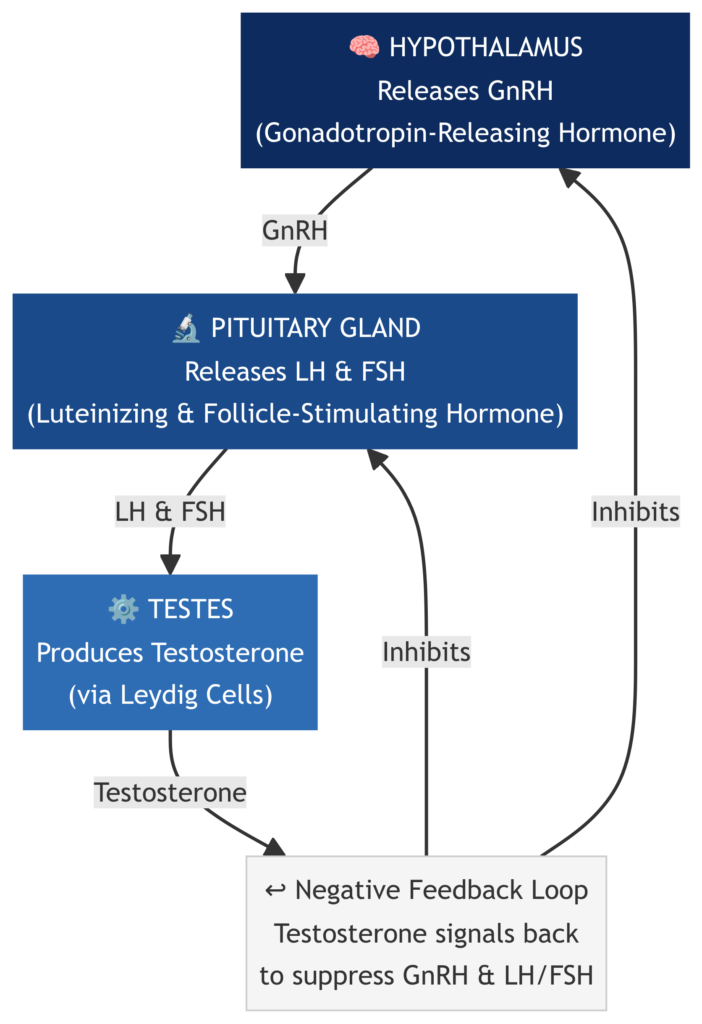
The hypothalamus releases Gonadotropin-Releasing Hormone (GnRH), which signals the pituitary gland to release Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH). LH then stimulates the Leydig cells in the testes to produce testosterone.
Unfortunately, natural testosterone production is not static. Clinical data indicates that testosterone levels generally peak during early adulthood and begin a gradual decline of approximately 1% to 2% per year after the age of 30 . This age-related decline, combined with modern environmental factors, stress, and poor metabolic health, has led to an epidemic of sub-optimal testosterone levels.
When the body can no longer produce adequate testosterone—a condition known as hypogonadism—the introduction of exogenous testosterone via TRT becomes a medical necessity to restore physiological function and quality of life.
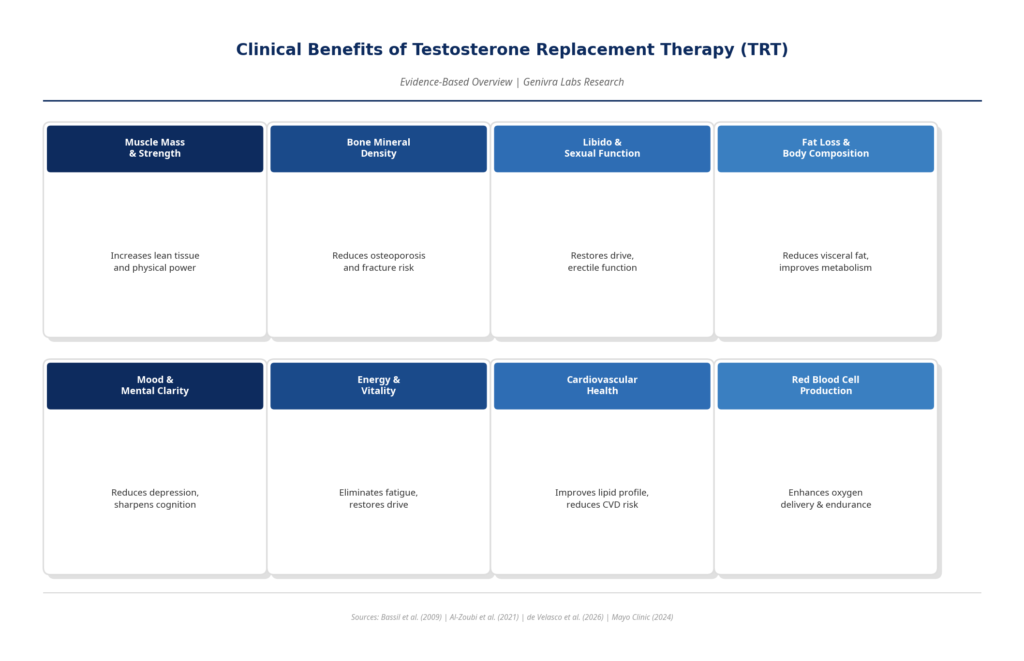
The Clinical Benefits of Optimized Testosterone
The therapeutic application of testosterone yields systemic benefits that extend far beyond muscle growth. Extensive clinical trials and retrospective cohort studies have documented the transformative effects of restoring testosterone to optimal physiological ranges.
1. Body Composition and Metabolic Health
One of the most immediate and visible effects of TRT is a profound shift in body composition. Testosterone is a potent regulator of metabolism. Clinical studies demonstrate that TRT significantly reduces body weight, waist circumference, and fat mass while simultaneously increasing lean muscle tissue . Furthermore, optimized testosterone improves insulin sensitivity and glycemic control, directly reducing the risk factors associated with metabolic syndrome and type 2 diabetes .
2. Cardiovascular Function
Historically, the relationship between testosterone and cardiovascular health was misunderstood. However, modern, large-scale reviews indicate that TRT can actually reduce the risk of cardiovascular disease (CVD) in hypogonadal men. By improving lipid profiles, reducing visceral fat, and enhancing endothelial function, TRT addresses several root causes of cardiovascular pathology . While some retrospective studies have shown conflicting results, the consensus among longevity specialists is that maintaining testosterone in the upper physiological range is cardioprotective.
3. Bone Mineral Density
Testosterone plays a critical role in bone remodeling. As men age and testosterone declines, the risk of osteopenia and osteoporosis increases significantly. TRT has been shown to increase bone mineral density, particularly in the lumbar spine, thereby reducing the risk of frailty and fractures in later life .
4. Cognitive Function, Mood, and Vitality
The brain is dense with androgen receptors. Men suffering from low testosterone frequently report symptoms of depression, brain fog, chronic fatigue, and a lack of motivation. Restoring testosterone levels has a profound neuroprotective effect, improving mood, sharpening cognitive focus, and restoring a general sense of vitality and drive .
5. Sexual Health and Libido
Perhaps the most well-known benefit of TRT is the restoration of sexual function. Evidence consistently demonstrates that TRT improves sexual desire, erectile function, and overall sexual satisfaction, which are critical components of male well-being .
Modern TRT Protocols: Clinical vs. Sports Optimization
The approach to TRT dosing has evolved significantly. The outdated model of massive, infrequent injections (e.g., every 2 to 4 weeks) leads to severe hormonal fluctuations—spiking estrogen and causing mood crashes. Modern protocols prioritize stability above all else. Equally important is the choice of testosterone ester, as different formulations have fundamentally different pharmacokinetic profiles, injection frequencies, and ideal patient populations.
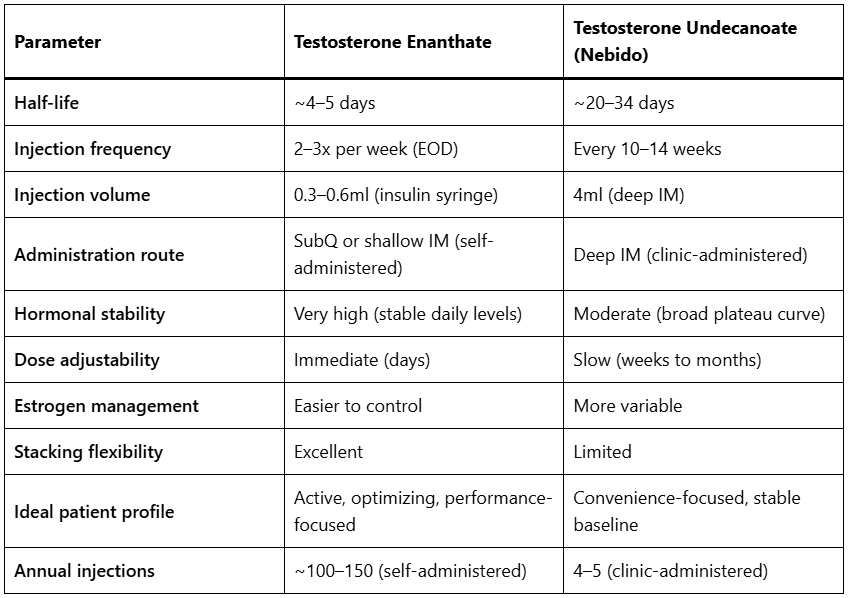
Choosing Your Testosterone Ester: Enanthate vs. Undecanoate (Nebido)
At Genivra Labs, we recognize that no single formulation is universally optimal. The two most clinically relevant injectable testosterone esters for long-term TRT are Testosterone Enanthate and Testosterone Undecanoate (Nebido). Understanding the pharmacological differences between them is essential for selecting the protocol that best aligns with your lifestyle, goals, and physiology.
Testosterone Enanthate — Precision and Control
Testosterone Enanthate is a medium-to-long acting ester with a half-life of approximately 4 to 5 days. This relatively short half-life is, paradoxically, one of its greatest clinical advantages: it allows for precise, frequent micro-dosing that closely mimics the body’s natural pulsatile testosterone secretion pattern.
When administered every other day (EOD) or twice weekly using a fine insulin syringe, Testosterone Enanthate produces exceptionally stable serum testosterone levels with minimal peak-to-trough fluctuation. This stability is critical for minimizing estrogen conversion (aromatization), preventing water retention, and ensuring consistent mood, energy, and libido throughout the week. The ability to self-administer subcutaneously (into the fat layer beneath the skin) makes this protocol highly accessible and virtually painless.
For individuals who are actively optimizing their hormonal profile, tracking biomarkers, or stacking with other compounds such as peptides or Masterone-E, Testosterone Enanthate provides the granular control necessary to fine-tune the protocol in response to blood work results.
Standard Protocol:
• Dosage: 100mg to 170mg per week (divided into EOD or twice-weekly injections)
• Administration: Subcutaneous (SubQ) or shallow intramuscular (IM) using an insulin syringe into the deltoid, gluteus, or abdominal fat
• Ideal for: Active individuals, athletes, biohackers, those who prioritize hormonal stability and protocol flexibility
Testosterone Undecanoate (Nebido) — Convenience and Long-Term Stability
Testosterone Undecanoate, marketed under the brand name Nebido, represents the opposite end of the pharmacokinetic spectrum. It is an ultra-long-acting ester with a half-life of approximately 20 to 34 days, formulated as a 1,000mg/4ml intramuscular injection . Due to its exceptionally slow release from the injection depot in the muscle, a single Nebido injection maintains therapeutic testosterone levels for 10 to 14 weeks.
The clinical protocol for Nebido consists of an initial loading phase — typically two injections spaced 6 weeks apart — followed by maintenance injections every 10 to 14 weeks. This means a patient requires only 4 to 5 injections per year to maintain continuous TRT. The injections must be administered deep intramuscularly (typically into the gluteus maximus) by a healthcare professional, as the large injection volume (4ml) and viscous oil formulation are not suitable for self-administration.
Because of the slow, gradual release profile, Nebido produces a broad, relatively flat serum testosterone curve. While this avoids the sharp peaks associated with weekly injections, it also means that fine-tuning the protocol in response to blood work is considerably more difficult. If testosterone levels run too high or too low, the correction takes weeks to manifest — unlike Enanthate, where a dose adjustment is reflected in serum levels within days.
Standard Protocol:
• Dosage: 1,000mg (1 vial) every 10 to 14 weeks, following a 6-week loading injection
• Administration: Deep intramuscular injection (gluteus maximus), typically administered by a physician or nurse
• Ideal for: Men who prioritize convenience and minimal injection frequency; those who prefer clinic-administered TRT; individuals with stable, well-established hormonal baselines
Who Should Choose Testosterone Enanthate?
Testosterone Enanthate is the preferred choice for men who are actively engaged in their health optimization journey. If you are tracking blood work regularly, stacking with peptides or other compounds, participating in athletic training, or seeking the highest degree of hormonal stability and control, Enanthate’s short half-life and flexible dosing schedule make it the superior clinical tool. The ability to micro-dose subcutaneously with an insulin syringe removes the barrier of clinic visits entirely, empowering individuals to manage their own protocol with precision.
Who Should Choose Testosterone Undecanoate (Nebido)?
Nebido is ideally suited for men who have been on a stable TRT protocol for some time, have well-characterized hormonal responses, and prioritize convenience above all else. It is also a strong option for men who are uncomfortable with frequent self-injection or who prefer the oversight of a physician administering each dose. For men with confirmed hypogonadism who simply want to maintain a therapeutic testosterone level without the complexity of frequent dosing, Nebido provides a highly effective and clinically validated solution .
The Standard Clinical Protocol (Testosterone Enanthate)
For general health and longevity, the goal is to maintain stable blood serum levels in the upper quartile of the natural reference range (typically 800–1100 ng/dL).
• Compound: Testosterone Enanthate
• Dosage: 100mg to 150mg per week.
• Frequency: Administered via micro-dosing, typically split into two injections per week (e.g., every 3.5 days) or Every Other Day (EOD) using subcutaneous or shallow intramuscular injections.
Sports TRT and Performance Optimization
In the realm of athletics and high-performance optimization, “Sports TRT” refers to protocols designed to maximize recovery, strength, and musculoskeletal performance without crossing into supraphysiological, abusive steroid cycles.
• Dosage: 150mg to 200mg per week.
• Application: Athletes utilize these optimized levels to enhance erythropoiesis (red blood cell production for endurance), accelerate tissue repair, and maintain peak neurological drive during intense training blocks .
Synergistic Stacking: Peptides and TRT
While TRT provides the foundational hormonal environment for optimal health, its effects can be exponentially amplified when stacked with targeted peptide therapies. At Genivra Labs, we recommend specific combinations to address distinct physiological goals.
The Ultimate Recovery Stack: TRT + BPC-157
For athletes or individuals recovering from injuries, combining TRT with BPC-157 is highly effective. While testosterone provides the systemic anabolic environment, BPC-157 acts locally to accelerate the healing of tendons, ligaments, and muscle tissue. Studies show that BPC-157 upregulates growth hormone receptors in fibroblasts, making the tissue more responsive to repair signals .
• Protocol: Standard TRT + BPC-157 (250mcg injected locally near the injury site, twice daily).
The Longevity & Cellular Repair Stack: TRT + HGH + NAD+
For maximum anti-aging benefits, stacking TRT with Human Growth Hormone (HGH) and NAD+ creates a comprehensive cellular rejuvenation protocol.
• Testosterone maintains muscle mass and neurological drive.
• HGH (2 IU daily) promotes collagen synthesis, skin elasticity, and deep sleep.
• NAD+ restores mitochondrial function and cellular energy production.
The Advanced Recomp Stack: TRT + Masterone-E + Arimidex
For individuals seeking a lean, “dry,” and highly defined physique, managing estrogen is critical.
• Testosterone Enanthate: 150-170mg weekly.
• Masterone-E: 100-200mg weekly. Masteron binds strongly to SHBG (increasing free testosterone) and provides mild anti-estrogenic effects, resulting in dense, hard muscle tissue.
• Arimidex: 0.25mg to 0.5mg as needed to precisely control any excess aromatization and prevent water retention.
Managing Elevated Red Blood Cells (Erythrocytosis) on TRT
One of the most clinically significant side effects of long-term TRT is the stimulation of erythropoiesis — the production of red blood cells. Testosterone directly stimulates the kidneys to produce erythropoietin (EPO), which in turn signals the bone marrow to increase red blood cell production. While a moderate increase in red blood cell count is a normal and even beneficial response to TRT (improving oxygen-carrying capacity and endurance), excessive elevation can become a health risk.
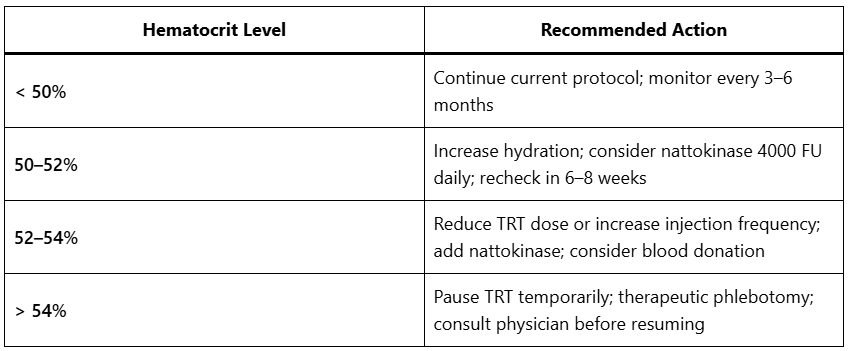
When hematocrit (the percentage of red blood cells in total blood volume) rises above 52–54%, the blood becomes significantly more viscous. This increased viscosity elevates the risk of thromboembolic events, including deep vein thrombosis (DVT), pulmonary embolism, and stroke. Regular blood work monitoring is therefore non-negotiable for anyone on long-term TRT — a full blood count (CBC) should be assessed at minimum every 3 to 6 months.
Practical Management Strategies
1. Dose Reduction and Injection Frequency Adjustment
The most direct intervention is to reduce the weekly testosterone dose or increase injection frequency. More frequent, smaller doses (EOD micro-dosing) reduce the peak serum testosterone spike, which is the primary driver of excessive erythropoiesis. Even a modest reduction from 200mg to 150mg weekly can normalize hematocrit within 8 to 12 weeks.
2. Therapeutic Phlebotomy (Blood Donation)
The most rapid and effective method for reducing hematocrit is therapeutic phlebotomy — simply donating blood. Removing 450–500ml of whole blood directly reduces the red blood cell mass and stimulates the body to produce fresh, less viscous blood. Regular blood donation (every 8 to 12 weeks if needed) is a well-established management strategy for TRT-induced erythrocytosis. It carries the additional benefit of contributing to public blood supply.
3. Hydration
Adequate hydration is often overlooked but critically important. Dehydration concentrates the blood, artificially elevating hematocrit readings. Ensuring a minimum of 3 to 4 litres of water daily can meaningfully reduce measured hematocrit and blood viscosity.
4. Nattokinase 4000 FU — A Natural Fibrinolytic Agent
Nattokinase is a serine protease enzyme derived from natto (fermented soybeans), and it represents one of the most compelling natural interventions for managing blood viscosity during TRT. Unlike pharmaceutical blood thinners, nattokinase works through a direct fibrinolytic mechanism — it breaks down fibrin, the protein scaffold of blood clots, and reduces the activity of plasminogen activator inhibitor-1 (PAI-1), thereby enhancing the body’s own clot-dissolving capacity.
At a dose of 4,000 FU (Fibrinolytic Units) daily, nattokinase has been shown in clinical research to reduce blood viscosity, lower fibrinogen levels, and improve microcirculation without the bleeding risks associated with pharmaceutical anticoagulants. For individuals on TRT with borderline-elevated hematocrit (50–54%), nattokinase 4000 FU taken daily — ideally on an empty stomach in the morning — serves as a highly effective, evidence-supported cardiovascular protective measure.
Important note: Nattokinase should not be combined with pharmaceutical anticoagulants (warfarin, heparin, direct oral anticoagulants) without medical supervision, as additive effects may increase bleeding risk.
Hematocrit Management Summary
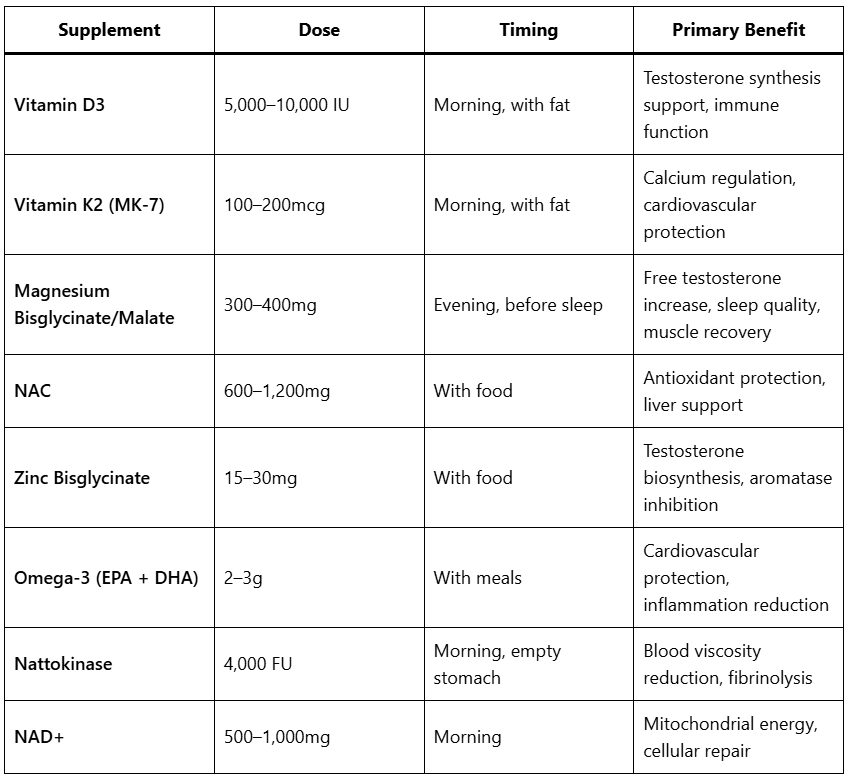
Essential Supplementation During TRT
Testosterone optimization does not exist in isolation. The hormonal shifts induced by TRT create specific micronutrient demands that, if left unaddressed, can blunt the benefits of therapy and contribute to long-term health risks. At Genivra Labs, we consider the following supplements to be foundational components of any comprehensive TRT protocol.
Vitamin D3 + K2 (MK-7)
Testosterone and Vitamin D3 share a deeply intertwined relationship. Vitamin D3 functions not merely as a vitamin but as a steroid hormone precursor, and androgen receptors throughout the body require adequate D3 for optimal function. Clinical studies consistently demonstrate that men with optimal Vitamin D3 levels (above 60 ng/mL) have significantly higher testosterone levels than those who are deficient. Furthermore, TRT increases calcium mobilization from bone, which makes Vitamin K2 (specifically the MK-7 form) indispensable — K2 directs calcium away from arterial walls and into bone tissue, protecting cardiovascular health during long-term TRT.
Recommended: Vitamin D3 5,000–10,000 IU daily + Vitamin K2 (MK-7) 100–200mcg daily, taken together with a fat-containing meal for optimal absorption.
Magnesium Bisglycinate or Malate
Magnesium is involved in over 300 enzymatic reactions in the body, including testosterone synthesis, protein synthesis, and neuromuscular function. Critically, magnesium competes with SHBG (Sex Hormone-Binding Globulin) for testosterone binding, meaning that adequate magnesium levels increase the proportion of free, bioavailable testosterone. Magnesium also plays a central role in sleep quality — deep, restorative sleep is the primary window for growth hormone secretion and cellular repair, making it essential for maximizing TRT outcomes.
Of the available forms, magnesium bisglycinate offers the highest bioavailability and the best gastrointestinal tolerability, while magnesium malate provides additional support for mitochondrial energy production (ATP synthesis), making it particularly beneficial for athletic individuals.
Recommended: 300–400mg elemental magnesium daily, taken in the evening before sleep.
NAC (N-Acetyl Cysteine)
N-Acetyl Cysteine is the direct precursor to glutathione — the body’s master antioxidant. TRT increases metabolic rate and androgenic activity, which generates a higher oxidative load at the cellular level. NAC replenishes glutathione stores, providing robust protection against oxidative stress in the liver, cardiovascular system, and kidneys. Additionally, NAC has demonstrated hepatoprotective properties, which are particularly relevant for individuals who may be combining TRT with oral compounds or other supplements that place a burden on hepatic metabolism.
Recommended: 600–1,200mg NAC daily, taken with food.
Zinc Bisglycinate
Zinc is arguably the single most important mineral for male hormonal health. It is a direct cofactor in testosterone biosynthesis and a natural inhibitor of the aromatase enzyme — the enzyme responsible for converting testosterone into estrogen. Even mild zinc deficiency has been shown to significantly reduce testosterone levels and increase estrogen conversion. The bisglycinate form provides superior absorption compared to cheaper forms such as zinc oxide or zinc sulfate, and it avoids the gastrointestinal irritation commonly associated with high-dose zinc supplementation.
Recommended: 15–30mg zinc bisglycinate daily, taken with food. Avoid taking alongside high-dose calcium or iron, which compete for absorption.
Omega-3 Fatty Acids (EPA + DHA)
Omega-3 fatty acids are essential for cardiovascular health, inflammation regulation, and cellular membrane integrity. In the context of TRT, their importance is amplified for several reasons. First, testosterone therapy can modestly increase LDL cholesterol in some individuals — Omega-3s (particularly EPA) counteract this by reducing triglycerides and improving the LDL particle size profile. Second, EPA and DHA reduce systemic inflammation and platelet aggregation, providing complementary cardiovascular protection alongside nattokinase. Third, DHA is a structural component of neuronal cell membranes, supporting the cognitive and mood benefits that TRT initiates.
Recommended: 2–3g combined EPA + DHA daily, from a high-quality, molecularly distilled fish oil or algae-based source. Take with meals.
Complete TRT Supplementation Protocol
Nutrition on TRT: Fuelling Hormonal Optimization
Testosterone Replacement Therapy creates a profoundly anabolic hormonal environment, but it cannot override the fundamental laws of nutrition. The quality of your dietary intake determines how effectively your body utilizes elevated testosterone levels — for tissue synthesis, metabolic function, and recovery. At Genivra Labs, we emphasize that TRT and nutrition are not separate variables; they are deeply interdependent. A poorly structured diet will blunt the benefits of even the most precisely calibrated TRT protocol.
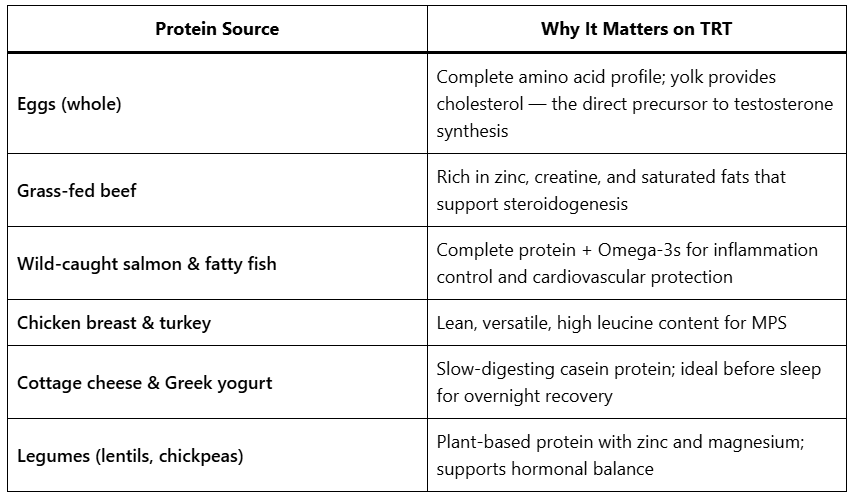
Protein: The Structural Foundation
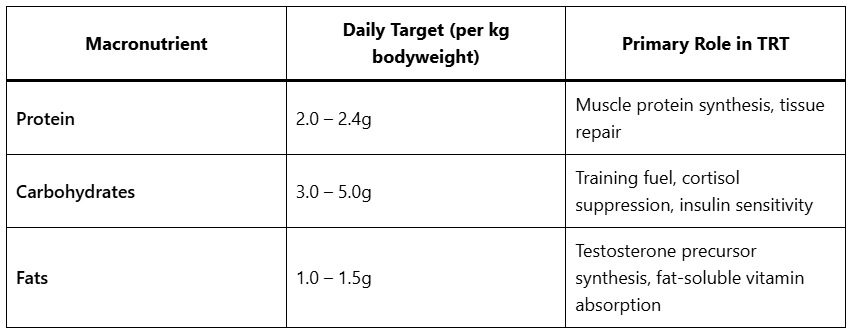
Protein is the macronutrient most directly linked to the anabolic effects of testosterone. Testosterone increases the rate of muscle protein synthesis (MPS), but only when sufficient dietary protein is available as the raw material. For individuals on TRT, a daily protein intake of 2.0 to 2.4g per kilogram of body weight is recommended to fully capitalize on the enhanced anabolic signalling.
The emphasis should be on complete, high-quality protein sources that provide all essential amino acids, particularly leucine, which acts as the primary trigger for MPS:
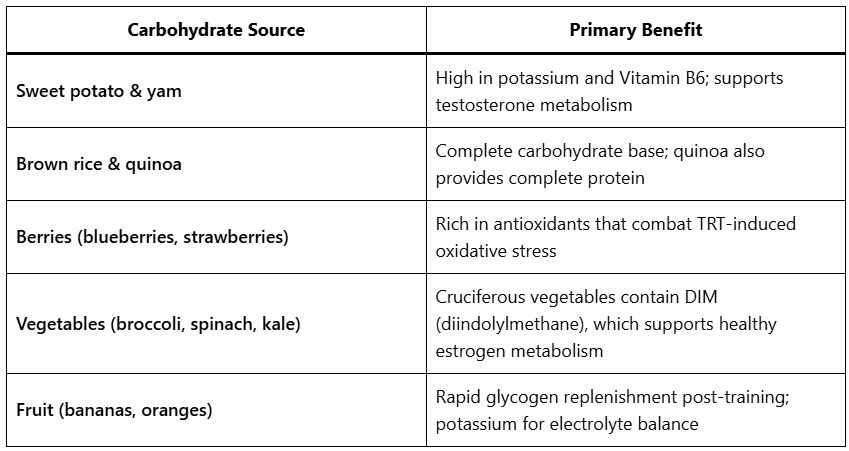
Carbohydrates: Energy, Cortisol Management, and Insulin Sensitivity
Carbohydrates are the primary fuel source for high-intensity training and play a critical but often misunderstood role in hormonal health. Chronically low carbohydrate intake elevates cortisol — the catabolic stress hormone that directly antagonizes testosterone. Adequate carbohydrate intake keeps cortisol suppressed, protects muscle tissue, and ensures the glycogen stores necessary for productive strength training.
The focus should be on low-glycaemic, nutrient-dense carbohydrate sources that provide sustained energy without causing insulin spikes that promote fat storage:
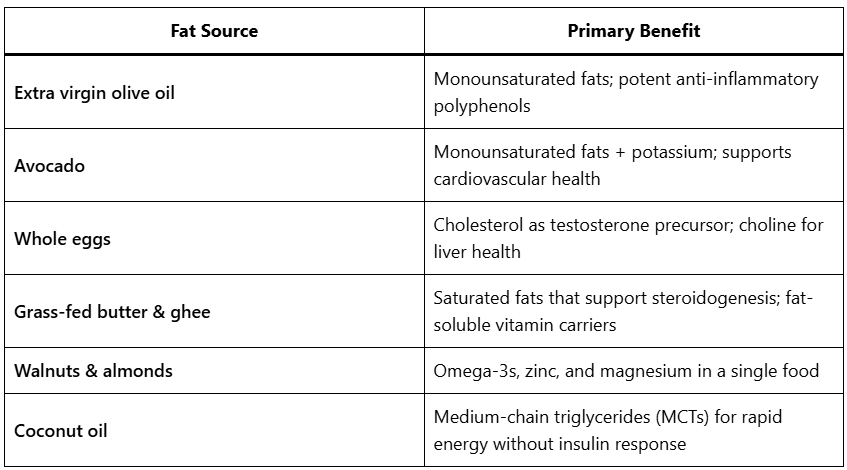
Fats: The Hormonal Raw Material
Dietary fat is arguably the most critical macronutrient for testosterone production. Testosterone is a steroid hormone synthesized from cholesterol, and chronically low dietary fat intake has been directly correlated with reduced testosterone levels. Men on TRT still benefit from adequate dietary fat, as it supports the endogenous hormonal environment and the metabolism of fat-soluble vitamins (D3, K2) that are essential to the protocol.
The distinction between fat types is critical: saturated and monounsaturated fats support testosterone synthesis, while trans fats actively suppress it.
Practical Macronutrient Guidelines
Training on TRT: Strength, Conditioning, and Cardio Zone Strategy
TRT fundamentally alters the body’s capacity for training adaptation. Elevated testosterone accelerates recovery between sessions, increases the rate of muscle protein synthesis, enhances neuromuscular drive, and improves the anabolic response to resistance training. However, to fully exploit these advantages, training must be structured intelligently. Indiscriminate high-volume training without periodization will lead to overreaching, elevated cortisol, and paradoxically blunted results.
Strength Training: The Primary Driver of TRT Benefits
Resistance training is the most potent non-pharmacological stimulus for testosterone receptor upregulation. When combined with TRT, structured strength training produces synergistic results that neither intervention achieves independently. The elevated testosterone environment created by TRT amplifies the muscle protein synthesis response to each training session, while the training itself increases androgen receptor density in muscle tissue, making the body more sensitive to the testosterone being administered.
Optimal Strength Training Structure on TRT:
The most effective approach for individuals on TRT is a 3 to 5 day per week strength training programme built around compound, multi-joint movements. These exercises recruit the largest muscle groups and generate the greatest hormonal response:
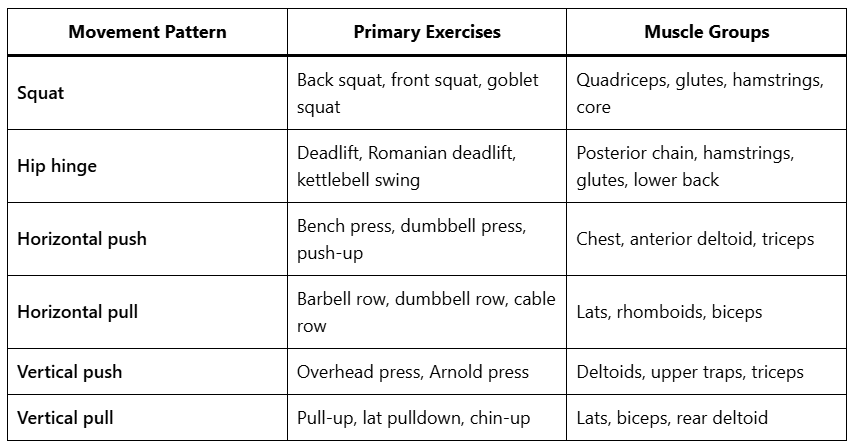
Recommended Training Parameters:
• Sets per session: 15 to 25 working sets
• Rep ranges: 3 to 6 reps (maximal strength), 6 to 12 reps (hypertrophy), 12 to 20 reps (metabolic/endurance)
• Rest periods: 2 to 4 minutes for compound lifts; 60 to 90 seconds for isolation work
• Progressive overload: Increase load or volume by 2 to 5% weekly to ensure continued adaptation
• Training frequency: Each muscle group should be trained 2 times per week for optimal hypertrophic stimulus
Cardiovascular Training: The Three-Zone Model
Cardiovascular training on TRT serves multiple purposes beyond caloric expenditure: it improves cardiac output, enhances mitochondrial density, manages hematocrit by improving blood fluidity, and accelerates recovery between strength sessions. The key to effective cardio on TRT is zone-based training — understanding that different heart rate zones produce fundamentally different physiological adaptations.
Heart rate zones are calculated as a percentage of your Maximum Heart Rate (MHR), estimated as: MHR = 220 – age.
Zone 1 — Active Recovery and Aerobic Base (50–60% MHR)
Zone 1 is low-intensity, conversational-pace exercise. At this intensity, the body relies almost exclusively on fat oxidation for fuel, and the cardiovascular system operates well below its capacity. The primary purpose of Zone 1 training on TRT is active recovery — it increases blood flow to muscles, accelerates the clearance of metabolic waste products (lactate, hydrogen ions), and promotes parasympathetic nervous system activation, which reduces cortisol and enhances recovery.
For individuals on TRT with elevated hematocrit, Zone 1 cardio is particularly valuable: the increased cardiac output at low intensity improves blood fluidity and microcirculation without placing excessive stress on the cardiovascular system.
Zone 1 Applications:
• 20 to 45 minutes of walking, light cycling, or swimming on rest days
• Morning fasted walks (20–30 minutes) to enhance fat oxidation and cortisol regulation
• Post-strength-training cool-down (10–15 minutes)
• Frequency: 3 to 5 times per week, on rest days or as active recovery
Zone 2 — Aerobic Efficiency and Metabolic Health (60–70% MHR)
Zone 2 is the most scientifically validated training zone for long-term metabolic health and cardiovascular adaptation. At this intensity, the body is working at the upper limit of pure aerobic metabolism — primarily burning fat, with minimal lactate accumulation. Sustained Zone 2 training drives profound mitochondrial biogenesis (the creation of new mitochondria), increases the density of oxidative muscle fibres, and dramatically improves insulin sensitivity.
In the context of TRT, Zone 2 training is a powerful complement to the metabolic improvements that testosterone initiates. It enhances the body’s capacity to oxidize fat, reduces visceral adipose tissue, and improves cardiovascular efficiency — all of which amplify the body composition benefits of the protocol. Critically, Zone 2 does not significantly elevate cortisol, making it compatible with high-frequency strength training without compromising recovery.
Zone 2 Applications:
• 30 to 60 minutes of steady-state cycling, jogging, rowing, or elliptical
• The “talk test”: you should be able to speak in full sentences but feel mildly breathless
• Frequency: 2 to 4 times per week; 3 hours of Zone 2 per week is the evidence-based minimum for meaningful mitochondrial adaptation
Zone 3 — Lactate Threshold and High-Intensity Conditioning (70–85% MHR)
Zone 3 represents moderate-to-high intensity training where the body begins to rely increasingly on anaerobic glycolysis. At this intensity, lactate begins to accumulate faster than it can be cleared, and the cardiovascular and respiratory systems are working at significant capacity. Zone 3 training improves lactate threshold (the point at which fatigue accelerates), increases VO2max, and develops the kind of cardiovascular conditioning that directly translates to athletic performance.
For individuals on TRT, Zone 3 training should be used strategically rather than as the default cardio modality. While it is highly effective for improving athletic capacity, it generates significant cortisol and requires adequate recovery time. The elevated testosterone environment of TRT accelerates recovery from Zone 3 sessions, but excessive Zone 3 volume without sufficient Zone 1 and Zone 2 base work can lead to overtraining and hormonal dysregulation.
Zone 3 Applications:
• Tempo runs, cycling intervals, rowing ergometer intervals
• Circuit training with moderate loads and short rest periods
• HIIT sessions (High-Intensity Interval Training) — 20 to 30 second efforts with 1 to 2 minute recovery
• Frequency: 1 to 2 times per week maximum; always separated by at least 48 hours of recovery
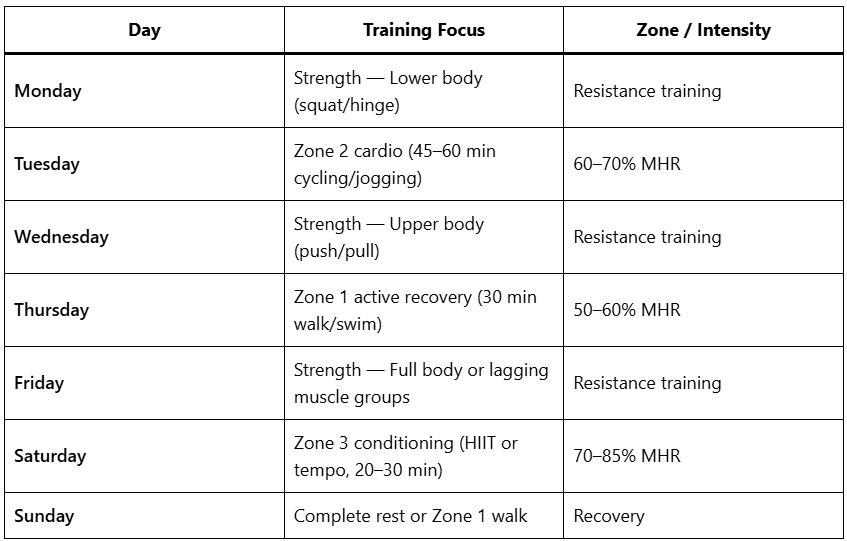
Recommended Weekly Training Structure on TRT
Sleep, Stress, and Cortisol Management: The Invisible Variables
Testosterone Replacement Therapy provides the hormonal foundation, but the body’s ability to utilize that testosterone is heavily dependent on two critical lifestyle factors: sleep architecture and stress management. Ignoring these variables will severely blunt the efficacy of any TRT protocol.
Sleep Architecture and Hormonal Output
While exogenous testosterone (TRT) provides a stable baseline, the body’s endogenous production of complementary hormones — particularly Human Growth Hormone (HGH) and melatonin — is entirely dependent on sleep quality. The majority of daily HGH secretion occurs during the first cycle of deep, slow-wave sleep (SWS). Furthermore, chronic sleep deprivation (less than 6 hours per night) has been shown to increase cortisol levels by up to 50% the following evening, creating a highly catabolic environment that directly antagonizes the anabolic effects of TRT.
Optimization Strategies:
• Circadian alignment: Maintain a consistent sleep/wake schedule, even on weekends, to anchor your circadian rhythm.
• Temperature regulation: The core body temperature must drop by approximately 1°C to initiate deep sleep. Keep the bedroom cool (18–20°C) and consider a warm shower 90 minutes before bed to trigger the cooling response.
• Light management: Block blue light exposure 2 hours before sleep (using blue-blocking glasses or software filters) to allow natural melatonin production.
Cortisol and the Autonomic Nervous System
Cortisol is the body’s primary stress hormone. While acute cortisol spikes are necessary for training adaptation and morning wakefulness, chronically elevated cortisol — driven by psychological stress, overtraining, or poor diet — is highly destructive. Cortisol and testosterone share the same precursor molecule (pregnenolone). In states of chronic stress, the body prioritizes cortisol production over sex hormones, a phenomenon known as the “pregnenolone steal.”
Even on TRT, where testosterone levels are artificially maintained, high cortisol will bind to glucocorticoid receptors in muscle tissue, promoting protein breakdown and fat storage (particularly visceral fat).
Optimization Strategies:
• Breathwork: Implement 5–10 minutes of resonance frequency breathing (e.g., 5 seconds inhale, 5 seconds exhale) daily to shift the autonomic nervous system from sympathetic (fight-or-flight) to parasympathetic (rest-and-digest) dominance.
• Adaptogens: Consider supplementing with Ashwagandha (KSM-66) or Rhodiola Rosea, which have been clinically shown to reduce serum cortisol levels and improve stress resilience.
Estrogen Management and Aromatization
One of the most critical aspects of a successful TRT protocol is the management of estradiol (E2). Testosterone is naturally converted into estradiol by the aromatase enzyme, which is found primarily in adipose (fat) tissue. While estrogen is often unfairly demonized in men’s health circles, it is absolutely essential for libido, joint health, cardiovascular protection, and cognitive function. The goal is not to eliminate estrogen, but to keep it in the optimal physiological ratio with testosterone.
The Symptoms of Estrogen Imbalance
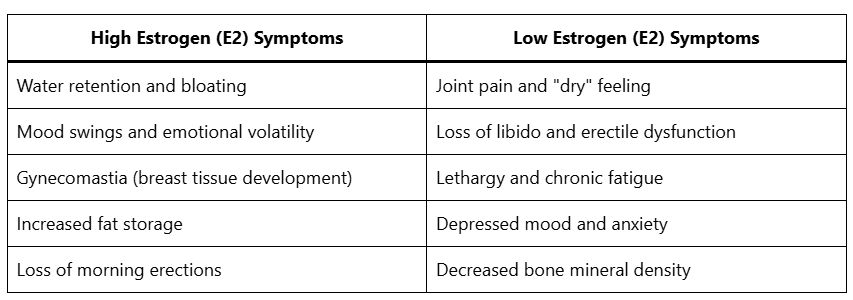
Management Strategies
- Protocol Optimization First: Before introducing pharmaceutical interventions, the first line of defense against high estrogen is optimizing the TRT protocol. Increasing injection frequency (e.g., moving from twice weekly to Every Other Day) reduces the peak testosterone spike, which directly reduces the rate of aromatization.
2. Body Composition: Because the aromatase enzyme is concentrated in fat tissue, reducing body fat percentage is the most effective long-term strategy for controlling estrogen conversion.
3. Aromatase Inhibitors (AIs): If symptoms of high estrogen persist despite protocol optimization, a low-dose Aromatase Inhibitor such as Arimidex (Anastrozole) may be necessary. The dosing must be extremely conservative — typically 0.25mg to 0.5mg taken 1 to 2 times per week, ideally on the day of the testosterone injection. Over-inhibition of estrogen is highly detrimental and must be avoided.
Fertility and Testicular Function on TRT
A common misconception is that TRT acts as a male contraceptive. While exogenous testosterone does suppress the HPTA axis — leading to a significant reduction in Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH) — it does not guarantee infertility. However, long-term TRT will cause testicular atrophy (shrinkage) and a severe reduction in spermatogenesis (sperm production).
For men who wish to maintain fertility or testicular volume while on TRT, adjunctive therapies are required.
Human Chorionic Gonadotropin (HCG)
HCG is an analog of Luteinizing Hormone. When administered alongside TRT, it directly stimulates the Leydig cells in the testes, maintaining intra-testicular testosterone production, preserving testicular volume, and supporting spermatogenesis.
• Standard Protocol: 250 to 500 IU administered subcutaneously 2 to 3 times per week.
• Note: HCG increases aromatization, so estrogen levels must be monitored closely when adding it to a TRT protocol.
Clomiphene Citrate (Clomid) or Enclomiphene
For men coming off TRT to restore natural fertility, Selective Estrogen Receptor Modulators (SERMs) like Clomid or Enclomiphene are used to block estrogen receptors in the hypothalamus, tricking the brain into restarting GnRH, LH, and FSH production.
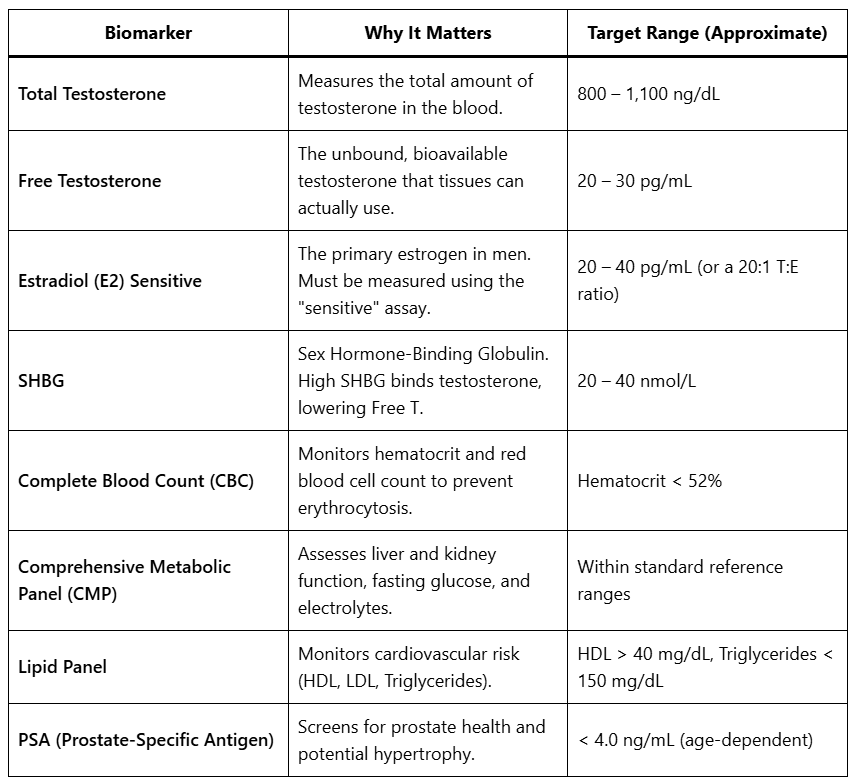
Blood Work and Biomarker Monitoring
TRT is a medical intervention that requires objective data. Subjective feeling is important, but it must be correlated with comprehensive blood work to ensure long-term safety and efficacy. Blood work should be conducted before initiating therapy (baseline), 6 to 8 weeks after any protocol change, and every 3 to 6 months once stable.
Essential TRT Biomarkers
Conclusion
Testosterone Replacement Therapy is no longer just about treating a deficiency; it is about optimizing the male machine. When administered correctly, with stable dosing protocols and high-quality compounds, TRT offers a profound improvement in body composition, cardiovascular health, cognitive function, and overall vitality. By integrating advanced peptide therapies like BPC-157 and HGH, individuals can push the boundaries of recovery and longevity.
Disclaimer: Hormone optimization requires careful monitoring. We strongly recommend regular comprehensive blood work and consultation with a qualified healthcare professional before beginning any TRT or peptide protocol.